First Published : March 2026
Latest Update : May 2026
Copyright © 2026 by Sarovah Healthcare
Authors
Written by Sumeet Moray for Sarovah Healthcare
What is the “Community Owned Healthcare” ?
Why is our Healthcare so affordable ?
Benefits over Private Healthcare
Benefits over Government Healthcare
Benefits over Private Health Insurance
Benefits for Healthcare Workers
Facilities in the Community Healthcare System
Certifications & Measures for Quality Assurance
Hospital Capacity Metrics in Detail
Real world Case Studies and Healthcare Models(Incomplete)
Long Term Planning & System Design (Incomplete)
Phase Wise Funding and Development Plan
Ideas & Options for Fundraising
Appreciation for the Founding Members
Frequently Asked Questions (FAQs)
Create a Healthcare community in your City
“Community Owned Healthcare” is a healthcare system where the community funds and owns its own hospitals & healthcare facilities under the guidance of healthcare professionals, doctors and industry veterans.
The healthcare system is owned by the Community. The community of people like you. Not by shareholders. Not by profit seeking corporations.
Legally it is registered as a healthcare cooperative - a nonprofit cooperative society.
Because the community owns its own hospitals it can vote for the policy decisions. The community can ensure that the system is designed to care for the patients & healthcare workers. The system is honest and the system respects the ethics of healthcare.
This allows the doctors and healthcare workers the freedom to practice ethical healthcare. Because they are not under any pressure from the corporate system to maximize profits at the cost of healthcare ethics.
Doctors and Healthcare workers get the freedom to practice what they love. Which is to heal patients & care for them.
The problem with traditional cooperatives is that after sometime they start to feel like a government department rather than a community. We take a very different approach to ensure that our community continues to feel like a community and does not evolve into a government department.
At Sarovah Healthcare we embrace modern technology. Members can use our mobile app to vote for decisions, organize offline meetups / events / workshops, discussions within the community happen on our mobile app, our app has a finance tracker where members can track how the community funds are spent with proper photo and video evidence.
Booking doctor appointments, booking tests & scans, keeping health records and more also happen through our mobile app.
Because the community members can vote for the decisions from the comfort of their mobile phones. The management cannot force non-democratic decisions on the community. We have a policy to maintain a proper photo and video evidence for each and every financial transaction. Members can view all the financial records on the mobile app. Due to this corruption becomes very difficult.
Use of technology ensure’s that community remains truly democratic where each and every member can raise & discuss their concerns with the community. It also helps ensure that the community remains financially transparent and bureaucracy is eliminated.
Legally the community is registered as a Nonprofit Cooperative Organization. When you join our community you become the member of this cooperative society.
Not every cooperative is a Nonprofit but ours is a Nonprofit by choice.
The staff is paid on a salary basis. But the community does not generate any profits or surplus for its members. This is done intentionally to ensure that there are no compromises in the ethics of healthcare.
In this section we will see membership plans and payment structures.
When you’re building your home you would need a one time investment for the construction of your home. In business terminology we call it CAPEX - Capital Expenditure.
We charge a one time fee to generate funds required for the construction of hospitals and buying expensive medical equipment. This is paid only once.
Once you pay this fee you become the owner of the Community hospitals. You can now vote with your community for policy & management decisions of your hospitals because you are the owner.
This fee is transferable which means if you’re moving to another city or want to leave the community for any reason. You can apply for membership transfer. Your membership will be transferred to a new member and you will get a refund.
Once you have built your home. You now need some money for the routine maintenance of your home. The maintenance would include things like electricity, cleaning, repair, etc.
In business terminology we call it OPEX - Operational Expenditure.
Members can choose to pay for their routine healthcare needs using one of the two following options. This helps us recover the operational costs of the hospital & pay salaries to the hospital staff.
Members can choose to pay out of pocket.
Members can expect to save 50 - 70 % in their hospital bills compared to private healthcare. Please see the full price comparison chart (given in the next chapter) for estimated member prices and how member prices differ from market prices.
The prices for members are much lower and affordable than private hospitals because we only recover the operating costs. The cost for hospital building and expensive equipment has already been paid for. And due to Nonprofit legal structure we don’t have profit obligations.
Members can choose to opt for a yearly subscription of Rs. 10000 per year.
This subscription covers almost all healthcare needs - doctor consultations, OPD, Medicines, Scans like - MRI / CT/ Ultrasound / X-Ray, Pathology tests like CBC, Lipid Profile, etc, IPD & ICU admission’s, and even surgeries
Subscription prices can vary with age, health conditions but it will always be more affordable than private healthcare.
For private health insurance the more claims they deny the higher profits they make. So they are always looking for an excuse to deny a claim.
Your community hospital is a nonprofit. When we receive 100 rupees from our members. We are obligated to spend that entire 100 rupees on members' healthcare. We don't need to save that money to generate profits for our shareholders. The system gets no benefit from denying healthcare to their members.
Unlike private insurance there is no complicated discharge procedure - you get discharged immediately after any health procedure.
If you’re having difficulty deciding which option you want to go for. You can join the community and decide later. There is no pressure on members to make a choice at the time of joining. You can decide the options anytime and switch between the options as you like.
It is estimated that members can save roughly 50 -70 % in hospital bills when compared to private hospitals. Let us see an approximate comparison of the cost differences.
Note : These savings do not come from paying lower salaries to doctors and staff. In private hospitals only a small percent of what you pay go to the doctors and staff. These savings come primarily due to Nonprofit structure. And savings in the hospital expenses.
| Procedure | Private Hospital Rate | Cooperative Member Rate | Savings | Discount % |
|---|---|---|---|---|
| Normal Delivery | ₹60,000 – ₹80,000 | ₹25,000 | ₹45,000 | ~65% |
| C-Section Delivery | ₹1,00,000 – ₹1,30,000 | ₹45,000 | ₹70,000 | ~60% |
| Cataract Surgery (Mono) | ₹40,000 – ₹60,000 | ₹15,000 | ₹35,000 | ~75% |
| Laparoscopic Chole (Gallbladder) | ₹1,20,000 – ₹1,50,000 | ₹50,000 | ₹85,000 | ~65% |
| Angioplasty (Single Stent) | ₹2,50,000 – ₹3,50,000 | ₹1,10,000 | ₹1,90,000 | ~60% |
| Scan Type | Private Rate | Cooperative Member Rate | Savings (INR) | Savings % |
|---|---|---|---|---|
| MRI Brain (Single) | ₹7,000 – ₹9,000 | ₹2,200 – ₹2,800 | ₹5,500 | ~70% |
| CT Brain (Single) | ₹3,500 – ₹5,000 | ₹1,100 – ₹1,400 | ₹3,000 | ~75% |
| USG (Ultrasound) | ₹1,500 – ₹2,500 | ₹500 – ₹700 | ₹1,300 | ~70% |
| X-Ray (Chest) | ₹500 – ₹800 | ₹150 – ₹200 | ₹500 | ~75% |
| Whole Body CT | ₹15,000 – ₹18,000 | ₹4,500 – ₹5,500 | ₹11,500 | ~70% |
| Whole Body MRI | ₹20,000 – ₹23,000 | ₹7,000 – ₹8,500 | ₹14,000 | ~65% |
| Bed / Service Category | Market Rate (Private) | Cooperative Member Rate | Savings (INR) | Discount % |
|---|---|---|---|---|
| ICU / CCU Bed (Full Care) | ₹22,000 | ₹7,500 | ₹14,500 | ~66% |
| NICU Bed (Neonatal ICU) | ₹15,000 | ₹5,000 | ₹10,000 | ~66% |
| General Ward Bed | ₹2,500 | ₹800 | ₹1,700 | ~68% |
| Private AC Room | ₹9,500 | ₹3,200 | ₹6,300 | ~66% |
| Service | Market Rate (Private) | Cooperative Member Rate | Savings | Discount % |
|---|---|---|---|---|
| Dialysis (Single Session) | ₹3,500 | ₹1,100 | ₹2,400 | 68% |
| Chemotherapy (Session Fee) | ₹5,000 | ₹1,500 | ₹3,500 | 70% |
| Physiotherapy Session | ₹800 | ₹250 | ₹550 | 68% |
| Daycare Bed (6 Hours) | ₹2,000 | ₹500 | ₹1,500 | 75% |
Our members can expect to save roughly 50 - 70 % in their hospital bills.
We pay best in class salaries to our doctors to attract the best talent and we have world class medical facilities in our hospitals. So you may wonder how we can provide world class healthcare at such low and affordable costs ?
There are many reasons for that. Let us discuss them below.
Building hospitals is expensive and it needs very high capital investment. A 100 bed hospital roughly costs about rupees 60-90 crores to build in India in 2026. Most private hospitals raise this money either through Debt (Loans) or through Investors. If they take loans they have to pay Loan EMI’s with high interest rates. If they raise money through investors they have to give huge margins to investors.
When you get a bill in a private hospital that bill includes the cost of that loan EMI or investor margins.
In our community hospital a member pays a one time joining fee. This one time fee provides the money required for the construction of our hospitals. We don't have to pay any EMI on the loans and any margin to investors. We pass on these benefits to the members as a reduction in their Hospital bills.
A private hospital needs a high marketing budget to attract customers into the hospital and they need marketing on a regular basis.
In a community owned hospital our marketing costs are low. A community hospital already has thousands of members. The members have already paid money to build their own hospital. They are the owners of the hospital. Do we have to convince the owners to use their own hospital ? The answer is obvious.
Your private hospital bill includes added marketing costs. We pass on savings in marketing costs to our members as a reduction in hospital bills.
It is a well known fact that most private hospitals pay external doctors some commissions to refer customers to their hospitals or labs. Community hospitals do not need to pay commission to external doctors to refer patients to our hospitals. There are two reasons.
Reason 1 : We don't take outside (non-member) patients in our hospital. We do this to ensure that our hospitals are not overcrowded. Our hospitals give treatment only to members except for emergency cases. Because we don't take external patients we don't have to pay any referral commission to external doctors.
Reason 2 : Our hospitals are self-sufficient with all medical facilities. All the healthcare needs of the members are fully covered in our Healthcare System. So all the referrals in our hospital are internal referrals. Members don't need to get referred from outside to get treatment in our hospital.
Your private hospital bills include referral commissions. We don't have to pay referral commissions so we pass on the savings to our members.
We are legally registered as a Nonprofit Cooperative Organization. We don't have any obligation to generate any profits for our shareholders or owners. The owners are the members like you and members are not asking for any profits. Our members only ask for good quality healthcare.
Your private hospital bill includes the profits for shareholders of the hospital. We use part of our income to invest in the latest medical technology. And we pass on rest as savings to our members.
We are a legally registered Nonprofit Cooperative Society. So we are exempt from some corporate taxes as per the "Doctrine of Mutuality".
We pass on the tax savings as a reduction in hospital bills to our members.
Even if a hospital is built by a Nonprofit trust. Sometimes they get benefits from governments in the form of discounted land. These hospitals are legally bound to reserve some of their capacity to government quota patients.
In order to provide free healthcare to the government quota patients they have to charge higher costs to the non-quota patients.
We are hoping we don't have to ask the government for favors like discounted land. So we don't have to reserve any special government quota. We pass on the savings to our members.
Due to revenue and profit goals in private hospitals. They don't focus on preventative care. Because there is very less money to be made in preventative care. Community hospitals save a lot of money for members just by focussing on preventative care.
Let us understand this with an example. Sometimes a simple “homocysteine test” which costs 300-500 rupees can detect early signs of heart problems which may need expensive heart surgery costing lakhs in future. When a patient is made aware of the problems in advance, the patient can take measures to prevent problems in future.
In community hospitals doctors are encouraged to provide preventative care. This ensures that members don't have to go through expensive surgeries in future which can be prevented if problems are detected in early stages.
What members save from preventative care cannot be measured in money. It's more than just money. It's emotional and even psychological.
Not all Private Hospitals are corrupt. But there is an increasing trend of fraud and inflated pricing. A cooperative which is also a Nonprofit has zero incentive to commit pricing fraud & inflate hospital bills. The staff is paid a fixed salary. Their salary is not linked to the hospital bills. If you take this into account. The savings will increase further.
Savings due to different factors are summarized into a table.
| Benefit Category | Estimated Saving (%) | Why it Saves |
|---|---|---|
| Capital Servicing Cost | 10% – 15% | Eliminates high interest on bank loans and high margins for private investors by using interest-free member joining fees. |
| Marketing Costs | 8% – 10% | Removes the need for a high marketing budget, ads, and PR to attract "customers," as owners are the members. |
| Referral Commissions | 10% – 15% | Eliminates "cut practice" or commissions paid to external doctors by treating only members in a self-sufficient facility. |
| No-Profit Margin | 15% – 20% | Removes the profit targets required for shareholders; income is instead used for tech reinvestment or passed to members. |
| Corporate Taxes | 3% – 5% | Leverages the "Doctrine of Mutuality" to exempt the cooperative from certain corporate taxes that private hospitals must pay. |
| Charity Quota Loading | 10% – 12% | Avoids overcharging "paying" patients to cross-subsidize 20% free/concessional government-mandated beds. |
| Preventative Care | Varies (High) | Reduces long-term costs by detecting problems early (e.g., via homocysteine tests), preventing expensive future surgeries. |
| Total Savings | 50% - 70 % | Members are estimated to save 50% to 70% over private hospital bills. |
In the article we compare the benefits our members get compared to private healthcare.
Note : There will be some repetition of few points in this article. But that repetition is intentional to provide clarity in understanding.
In private healthcare doctors are usually given revenue targets. They constantly live in pressure and stress because if they fail to meet their targets they could lose their jobs.
Due to these targets they are sometimes forced to recommend procedures which they themselves feel may not be needed and necessary. A lot of doctors feel guilty about this because it's not something that they want to do.
Not all Private Hospitals are corrupt. But there is an increasing trend of fraud and inflated pricing in the private hospitals. A cooperative which is a Nonprofit has zero incentive to commit pricing fraud & inflate hospital bills. The staff is paid a fixed salary. Their salary is not linked to your hospital bills.
We have already discussed this in detail in the previous chapters. How a “Community Owned Healthcare” system can make healthcare more affordable for the average person.
In private healthcare the income of the doctors are often linked to the revenue they generate for the hospital.
We pay fixed salaries to our doctors. Even if the doctor does not recommend any procedure or test they are going to receive the same salary. This ensures that doctors would recommend something only when they feel it’s genuinely required for the patient.
In private hospitals doctors can have fixed salary but they can still be given targets to fulfill. Which can compromise the ethics of healthcare. Our system does not give any targets due to its cooperative and nonprofit structure.
Even when salaries are fixed we ensure that we offer the best in class salaries to make sure we attract the best talent in the industry.
Referral commission is considered illegal but it is still widespread in the medical industry. This corrupts the experience for the patient.
The system eliminates the practice of referral commissions because our system is self-sufficient in our healthcare facilities so all of our referrals are internal referrals.
In a private hospital a lot of doctors feel burned out due to being forced to fulfill multiple targets.
In our hospitals doctors are paid fixed salaries with no revenue targets. So doctors live in a stress free environment. Where their job is not to fulfill any targets but just to do what they love. Which is to provide better care for their patients.
Due to this doctors have better work life balance and they have better relationships with their patients.
Due to revenue and profit goals in private hospitals. They don't focus on preventative care. Because there is very less money to be made from preventative care.
Let us see that with an example. Sometimes a simple “homocysteine test” costing 300-500 rupees can detect early signs of heart problems which may need expensive heart surgery costing lakhs in future. When a patient is made aware of the problems in advance, the patient can take measures to prevent problems in future.
Because our hospitals are directly owned by the members. They can vote for policy decisions of the hospitals. Doctors in our hospitals are encouraged to provide preventative care for their patients.
This results in savings and benefits which go beyond money.
Let us discuss what kind of benefits our community hospital provides over government hospitals
Government hospitals are open for everyone. Which is a good thing but it can result in overcrowding.
We have a policy where we don't take outsiders (non-members) in our hospital except for emergency cases. This ensures that the hospitals are not overcrowded despite the affordable pricing.
There have been cases where cooperative hospitals have allowed non-members in their hospitals at higher prices to subsidize costs for members. But this causes overcrowding and degrades the quality of healthcare. Therefore we don't allow it.
As our core policy we don't allow non-members in our hospital to ensure that quality standards are maintained.
We are targeting a 100 bed hospital for 50000 members. This gives us 2 beds per 1000 people. The national average is 1.3 beds per 1000 people. This includes the private hospitals.
The ratio of 2 beds per 1000 people ensures that the experience at our hospitals will be better or at par with the best private hospitals in India.
When new members join we can put them on waitlist. And use their member contribution to build new hospitals. This ensures that we can always build more new hospitals to maintain a bed ratio of 2 beds per 1000 people.
Government hospitals are known to be ethical and affordable but they are known to be overcrowded and inaccessible. Private hospitals are accessible but they can be very expensive and unethical.
At “Community Owned Healthcare System” we find a balance. Where healthcare is ethical and affordable but also accessible to the common person.
It is a well known fact that government employees cant be removed from their job. This sometimes result in the staff lacking care for the customers and poor accountability towards their job and responsibilities. There are cases when they don’t do any work but still take the salary.
This happens because government cant remove the corrupt employees. Corrupt employees mostly get transferred or suspended. But they are rarely removed from the job. So there is no fear of bad service.
This is not a problem with cooperative because cooperative laws allow the cooperative to remove the employees similar to how they can be removed from any private company. If the community finds that a certain employee or a person in management is corrupt they can remove them easily with a notice period.
We provide a subscription option where our members get full health coverage for an annual subscription of just Rs. 10000. Let us see how our annual subscription option compares to private health insurance.
We provide full health coverage in an annual subscription starting at just Rs. 10000. Our coverage includes doctor consultations, OPD, medicines, IPD, ICU admissions, tests and scans, ambulance services, and even surgeries like heart surgery.
Private health insurance only covers hospital admissions. But it does not cover OPD, Medicines and lot of other things.
For private health insurance. The more claims they deny the higher profits they make. So they are always looking for an excuse to deny a claim.
Sometimes they even deny genuine claims and they use loopholes in the law to justify those rejections.
Our Community Hospital is a nonprofit organization. When we receive 100 rupees from our members we are obligated to spend all of that 100 rupees in the healthcare of our members. We get no incentive or benefit by saving money by denying claims.
When you receive treatment using private health insurance multiple parties are involved. So a patient has to go through a complicated discharge procedure at the end of their treatment.
We have no such complex discharge procedure. The patient is free to go as soon as their treatment is finished.
In private health insurance even when they provide you a cashless treatment facility. In the background the bills are negotiated and settled between multiple parties. This can sometimes manifest as extra friction or delays in approval. Or even part rejections in approvals.
In our annual subscription plan our system becomes the integrated care provider who is both the payer and the provider. So there are no need for approvals, negotiation and settlement needed between multiple parties. This makes the process very simple, smooth and hassle free.
Our annual subscription covers all treatments. Which means when you have paid an annual subscription we assume that you have already paid for all the treatment.
There is a real world example which demonstrate how such a system provides very good results for the patients.
Example : Kaiser Permanente is a healthcare Nonprofit with integrated care model. Members pay a monthly or annual subscription which covers all of their healthcare needs. In their system they are both the payer and care provider. Which means they own both the insurance (finance) department and hospitals.
This completely removes the friction between insurance and medicine. Their primary USP is the total lack of "out-of-network" billing surprises within their facilities; everything is pre-integrated and coordinated through one central organization.
In a private health insurance model. The hospitals have huge incentive to inflate bills. When they see that a patient has a health insurance. They would start finding excuses to inflate bills. Even if a procedure / test / scan is not genuinely required they will still recommend it to inflate the bill. This is well known in medical industry.
This creates a huge friction and conflict of interest between insurance companies and hospitals. Hospitals want to inflate bills while insurance companies want to deny claims and sometimes they deny even genuine claims. The patient suffers in their conflict.
In integrated care model this problem is eliminated. This hospital is both the payer and provider. The hospital has zero incentive to inflate bills because all of those bills will be paid from their own bank account. On the contrary the hospital has huge incentive to provide preventative care to ensure that problems are detected early so the costly procedures in the future can be avoided.
This is how the healthcare is supposed to be. The system works for the people. The system benefits from keeping people healthy. Not by keeping them sick or treating them in sickness.
Concerns over Misuse of “Integrated Care Model”
In “Integrated care model” the hospital benefits from reducing costs. So someone might raise a concern that the hospital might deny even genuine healthcare needs to reduce its costs. This can surely happen if the “integrated care model” is implemented in private healthcare. But the likelihood of this happening is very low in “Community Owned Healthcare” - A Healthcare Cooperative.
Because the entity who owns the system makes all the decisions. If the owners are shareholders they will surely want to reduce costs even by denying genuine healthcare needs.
But If the owners are patients themselves they would not want to reduce costs. Because most people want better healthcare over money. Yes money does matter but healthcare matters more. If your loved one is suffering and needs medical care. What would you prioritize more ? Healing your loved one or saving money for the hospital ?
In “Community Owned Healthcare” people (potential patients) vote for policy decisions. They will surely vote for policies which ensures that every person has access to healthcare. And nobody is denied access to genuine healthcare needs.
The system prioritize preventative care for the patients. Because when problems are detected early, expensive and costly procedures can be avoided. Helping the hospital reduce costs by avoiding an expensive surgery.
Doctors would recommend tests which they might not otherwise advise. All of these tests, scans and preventative measures are included in the annual subscription without any need to pay out of pocket for that.
Kaiser Permanente - a Healthcare Nonprofit with “integrated care model” is famous for their focus on Preventative Care. Their model demonstrates that integrated care model is very effective for preventative care.
Their integrated care model is the same model that we have adopted in our system. With some changes to suit for the Indian scenario.
Let us discuss the benefits doctors and healthcare workers get when they work in our system.
Most doctors & nurses enter this profession because they love to heal and care for their patients. But sometimes the system forces them to work for targets instead of their patients. This causes immense burnout in healthcare professions. Sometimes it also causes moral injury where doctors find themselves coping up with feelings of guilt and depression.
Our community hospital does not give any targets to our doctors and healthcare workers. Because our investments are already recovered from membership fees. There is no pressure on our hospital to hit any revenue or sales target.
Doctors and healthcare workers are free to pursue what they love.
Medical Staff receive fixed salaries for fixed working hours. Which means doctors & medical staff have more freedom in their work and have better work-life balance.
Community hospitals have an immense incentive to ensure that doctors are stress free and have a good work life balance. Because our target is better healthcare not the sales and revenue. If doctors and healthcare workers are burned out the quality of healthcare goes down with it. The system does not want that.
Even if we have low sales and low revenue our hospitals can survive because our investment is already recovered from the membership fees. Our only target is good healthcare, nothing else.
Doctors can do what they love without any pressure of meeting targets. This improves their relationship with their patients. Patients receive ethical care, better care which restores the trust in the doctors and fosters more respect for the medical staff.
Unlike government hospitals our hospitals are not overcrowded and doctors & medical staff gets sufficient time to establish good relationships with patients.
Improved relationship reduce burnout and foster long term happiness & satisfaction in the profession. Improved relationship helps you see yourself as a part of community not an employee.
Our community healthcare system will consist of one or multiple hospitals. The system will have these facilities. This is what we have planned. We can add more facilities at the request of the members.
Departments
OPD (Out Patient Department)
IPD (In Patient Department)
ICU (Intensive Care Unit)
Surgery and OT Complex
Radiology Department - MRI / CT /Ultrasound/ X-Ray
Pathology Department - Blood and Urine Tests
ER Department - 11 Bed Emergency Room
Labour and Delivery Suite (OB-GYN)
Mental Health Department
Dental Clinic and Dental Department
Pediatrics and Child Care
Infrastructure Facilities in the Hospital
Blood Storage Center - In house Blood Storage Center
Pharmacy (in-Patient and Out-Patient)
CSSD (Central Sterile Services Department) - The CSSD is a centralized unit within a healthcare facility that is responsible for the cleaning, disinfection, and sterilization of medical devices.
Dialysis Unit - 4-5 Dialysis Units for Kidney Patients
24/7 Emergency Ambulance - ALS (Advance Life Support Ambulance)
Support utilities
Dietary / Kitchen - To provide medically supervised meals to patients
Medical Gas Pipeline
STP (Sewage Treatment Plant) and ETP (Effluent Treatment Plant)
On-Premise Facilities
Four Wheeler Parking
Two Wheeler Parking
Other than medical facilities the system also provides many other facilities to the members to further improve their experience.
Members can book doctor appointments through the mobile app. This reduces the crowd and the waiting time for the patients in the hospital. You can just book an appointment on your mobile phone and arrive in the hospital 10 minutes before your appointment. No need to wait for an hour to meet your doctor.
Members can book tests and scans on their mobile apps. Similar to how you can book tests and scans on many private healthcare apps. But this one is dedicated for our healthcare system.
Members don’t need to visit the hospital to provide their blood or urine samples. The samples can be picked up from their homes and reports will be made available on the mobile app.
Lost a physical copy of your health record ? Your medical history ? Or Reports ? No need to worry. All the health records of the member will be available on the mobile app. This will include doctor appointments, their prescriptions. Tests, scans and reports. Members and even the doctors can access all the medical history of the patient on the app based computerized system.
Remember that this a “Community Owned Healthcare”. The community actively participates in all the important policy decisions. But voting through traditional ways can be very cumbersome and it can be discouraging. This can kill the spirit of democracy.
So we have app based voting feature. Members can vote for policy decisions through the comfort of their mobile app.
We have a policy that each and every financial transaction needs to be supported by a proper photo and video evidence. Records are available in public domain for all the members on the mobile app. This ensures that the members know how their funds are being spent. If they smell corruption they can investigate further.
Members can propose and organize offline meetups, events, workshops using our mobile app. Offline meetup and events are a very interesting way to engage with the community. App has the features to support and manage offline meetups, events and workshops.
The community can engage in discussions on our mobile app. This is very similar to WhatsApp group or a Reddit Community. This enables and supports the spirit of democracy within the community. If a member is having a problem they can share their problem or concerns with others on the online discussion forum.
The healthcare cooperative like us can have thousands of members and it can be very cumbersome to organize elections by traditional methods. We are working with the legal system to allow the community to organize their elections using the mobile app.
Please note even though we have an elected management the community has the full rights to vote for decisions. The management cannot force their decisions on the community. Management is only there is implement the decisions made by the community. In our system the management has no legal authority to force their decisions on the community. Because they are employees not the owners.
If the community feels that the management is corrupt or any person in the management is corrupt the community can vote to remove the management and call for re-elections anytime from the comfort of their mobile app.
The cooperative laws at this moment may not support app based elections but we are working with the government to bring this facility into our community.
Sometimes we don’t have an emergency but still a special care is needed for the transportation of patients. You cannot rely on taxi in such situations. We provide special patient transport which is trained and designed for the transportation of the patients who need extra care.
To ensure good quality healthcare we take certain policy measures and our hospitals target and comply with few certifications. Let us discuss them below.
Let us discuss various measures we take to ensure good quality healthcare at Sarovah Healthcare.
Sometimes a cooperative healthcare system may allow the treatment to non-members at higher costs to subsidize costs for members. But this has shown to result in overcrowding and this ultimately degrades the quality of healthcare.
So as a policy measure we do not allow treatment to non-members in our hospitals. Except for emergency cases where treatment is allowed on humanitarian grounds.
People who want to benefit from this system are always welcome to join as a member and be the part of community.
When new members join we put them on waiting list if we have exhausted our capacity. We use the money (joining fee) we get from new members to build new hospitals. This ensures that we can always build more new hospitals to ensure that there is no overcrowding. The way we see in government hospitals.
In India the national average is 1.3 beds per 1000 people. This includes the private hospitals. We target the bed ratio of 2 beds per 1000 people.
The ratio of 2 beds per 1000 people ensures that the experience at our hospitals will be better or at par with the best private hospitals in India.
For every 50000 people we will have a hospital with 100 beds. If more people join we can put them on a waitlist until the new hospital is constructed. This ensures that we never go below the bed ratio of 2 beds per 1000 people.
WHO recommends a bed ratio of 3:1000 but if we target that ratio. There is a good possibility that our hospital may remain underutilized which is a wastage of a useful resource. And the cost of healthcare will shoot up. So 2 beds per 1000 is a sweet-spot.
For the purpose of quality assurance our hospitals target and comply with these certifications.
NABH (National Accreditation Board for Hospitals & Healthcare Providers) accreditation is India's highest benchmark for hospital quality and patient safety, established by the Quality Council of India. It signifies that a healthcare facility adheres to strict, internationally recognized standards for patient care, safety, and operational efficiency.
A NABL certificate is an official recognition granted by the National Accreditation Board for Testing and Calibration Laboratories (NABL), verifying that a laboratory meets international quality standards (ISO/IEC 17025 or ISO 15189). It acts as a "stamp of approval" for technical competence, ensuring accurate, reliable, and globally accepted test results.
DNB (Diplomate of National Board) accreditation is a formal recognition granted by the National Board of Examinations in Medical Sciences (NBEMS) to hospitals allowing them to conduct postgraduate medical training.
While it is an educational certification, from a patient’s perspective, it serves as a powerful proxy for healthcare quality and safety
For a patient, a DNB-accredited hospital signifies that the facility has passed a rigorous audit of its infrastructure, staff, and clinical processes.
Verified High Standards: To be accredited, a hospital must meet strict criteria for bed strength, diagnostic equipment (like MRI/CT scans), and qualified full-time specialists. This ensures you are in a facility equipped to handle complex cases.
Constant Monitoring and Safety: Accredited hospitals are required to follow standardized clinical protocols. Studies show that accredited facilities often have lower incidences of medication errors and fewer postoperative infections due to stricter safety compliance.
24/7 Expert Coverage: DNB programs bring in qualified residents who provide round-the-clock medical cover. For a patient, this means there is always a trained doctor available to respond to emergencies or monitor recovery, overseen by senior consultants.
Evidence-Based Treatment: Because these hospitals are teaching centers, the medical staff must stay updated with the latest global guidelines and research. You are more likely to receive treatment based on current scientific "best practices" rather than outdated methods.
Better Communication and Ethics: The DNB curriculum emphasizes doctor-patient communication and ethical research. Patients often benefit from more detailed counseling regarding their treatment plans and discharge instructions.
DNB vs. NABH: A Brief Note
While DNB focuses on the hospital’s ability to teach and maintain clinical standards for training, NABH (National Accreditation Board for Hospitals) is a separate, purely patient-centric certification focused on safety and operational quality. Many top hospitals hold both, which is a "gold standard" indicating they excel in both teaching and patient safety.
Let us study the financial aspects of “Community Owned Healthcare” system.
To ensure good experience at our hospitals we will be targeting 2 beds per 1000 people.
The national average is 1.3 beds per 1000 people. This includes the private hospitals. So with the ratio of 2 beds per 1000 people. The crowd at our hospitals will be less than the average crowd at most private hospitals. The ratio of 2 beds per 1000 people ensures that the experience at our hospitals will be better or at par with the best private hospitals in India.
Most municipal planners in India aim for 2 beds per 1,000 people (which would be 100 beds for 50,000). Although in reality government is not able to achieve even 1 bed per 1000 people.
For an Indian healthcare scenario a ratio of 2 beds per 1000 people is considered a sweet spot to ensure that the hospital is not overcrowded and the hospital capacity is not wasted.
This means that we need a 100 bed hospital for every 50000 people. Or a 50 bed hospital for every 25000 people.
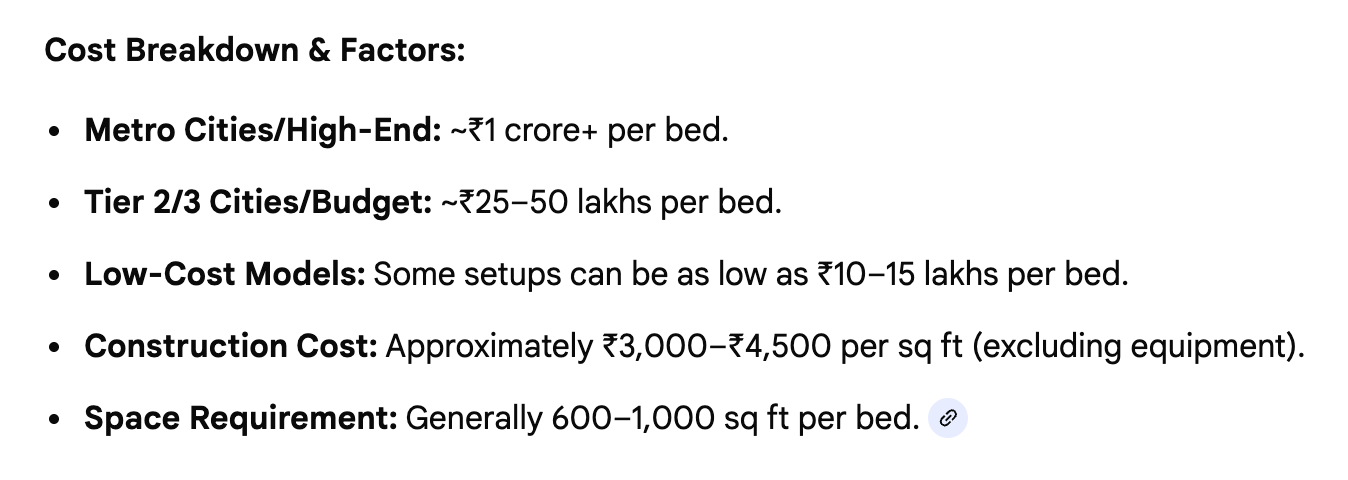
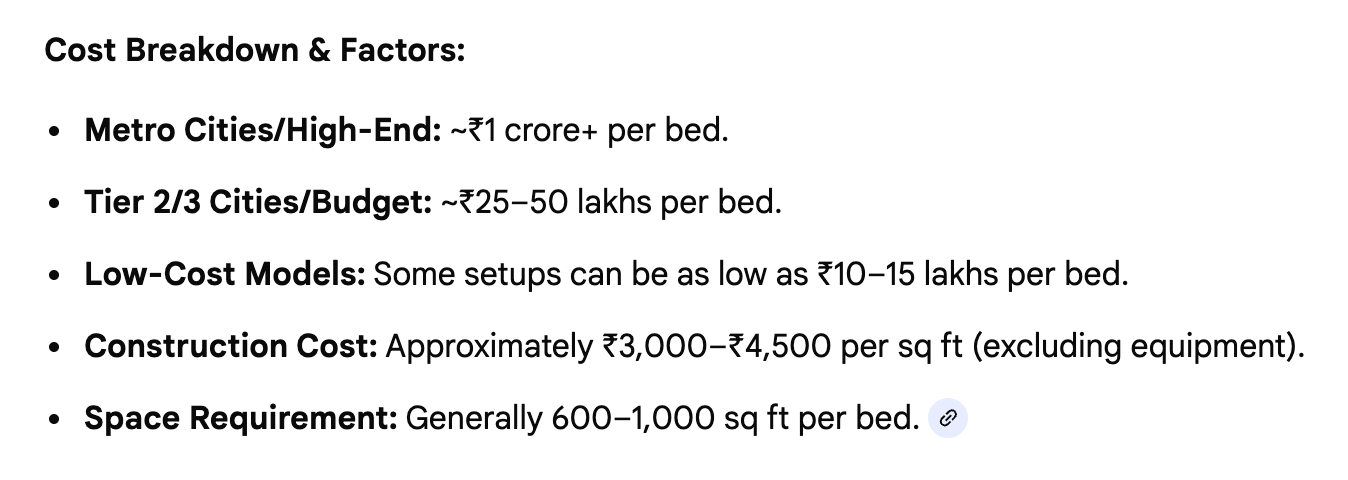
Based on current data as of 2026 the cost of construction of hospitals in city like Pune comes around 1 crore+ per bed. 1 crore per bed is still a conservative estimate the budget of high end private hospital goes above 2 crore+ per bed. But that hospital spends on lot on luxury aspects that has zero contribution in hygiene and quality of healthcare. So we don’t need that in our hospitals.
If we use our funds smartly by eliminating unnecessary luxury aspects and focussing only on healthcare essentials like high quality equipments and clean & hygienic premises in our hospitals. If we consider renting and renovating existing hospitals instead of building from scratch we can save a lot of our CAPEX budget. We can bring down our cost to 70 lakh per bed to 1 crore per bed.
This budget is enough for building a high quality NABH compliant hospital that adheres to international standards. This budget is enough for a hospital that will have high end equipment like MRI / CT / Ultrasound and NABL accredited lab.
If we aim for 2 beds per 1000 people. We need a CAPEX (Capital Expenditure) budget of 1.4 crore to 2 crore per 1000 people. This brings the per member contribution of 14000 to 20000 per member.
1.4 - 2 crore / 1000 people = 14000 to 20000 rupees per member
We need to account for some money for marketing, administrative costs also. Marketing is essential even if we are a cooperative. AMUL is a cooperative but they spend a lot of money on marketing. This shows that even if we are cooperative we must spend some money on marketing. It will surely be less than private healthcare but we cant eliminate the marketing budget.
We also need few months of working capital as a safety reserve to ensure smooth cash flow.
If we account for marketing, admin costs and safety reserve the estimate of 20000 per member sounds reasonable.
NCDC (National Cooperative Development Corporation) provides loans for cooperative initiatives. So as soon as we reach the mark of 25000 members we can start the hospital construction with the help of low interest Loan form NCDC.
Someone might ask if we are raising money from members why do we need Loans ?
We can have a scenario where we might have planned a hospital construction budget of Rs. 100 crores from 50000 members. But it is possible that right now we have only 30000 members who contributed Rs. 60 crores. In this scenario we will have to wait for more time to raise remaining Rs. 40 crores. In such a situation it would be better to raise that 40 crores from a loan and return that loan when we get remaining 40 crores from remaining 20000 members.
Time is a valuable asset. If the construction of the hospital gets delayed too much then people may lose interest. So starting the construction ASAP even with a loan is better than delaying too much. When the construction of the hospital begins it will become easier to attract new members because when people see the progress on the ground they are more interested.
We don't have to feel stressed about this loan because as soon as more members join the community we can return this loan easily. When people see a working hospital they are likely to be highly interested in joining the community. So this loan is not going to be a long term burden on the community.
After the construction of the hospital when people see a working hospital giving affordable healthcare. We will likely end up having a huge demand for new memberships. This will help us pay all the loan back in just 1-2 years.
In the long term we are hoping that we may find 2 to 2.5 lakh members in Pune. Which will give us enough funds to build 4-5 hospitals in Pune.
Having 4-5 hospitals in the city ensures that people don't have to travel very far and have easy access to the hospital near their homes.
Because members have already paid for the hospital construction we only have to recover operation costs from the members.
This helps us keep our costs 50-70 % lower than private healthcare.
The annual budget needed to run the 100 bed hospital hovers around 25 crores per year. The construction cost and land is already recovered with the joining fee. So we don't take it into the calculation.
The operational cost includes staff and doctor salaries and equipment AMC and more.
Out of 50000 members, if even 25000 members take our annual membership of Rs. 10000 per year it alone gives us a budget of 25 crores which is sufficient to cover annual operational costs of the hospital.
In this article we explain in more detail how we arrive at a figure of 100 bed hospital for 50000 people. You may skip this article if you don't want to go into details. This will help us understand how to plan our hospital capacity. And if a 100 bed hospital is sufficient for the population of 50000 people.
This will also help us understand how much investment (CAPEX) we need to raise to build our hospitals. And what will be the per member investment (CAPEX) share?
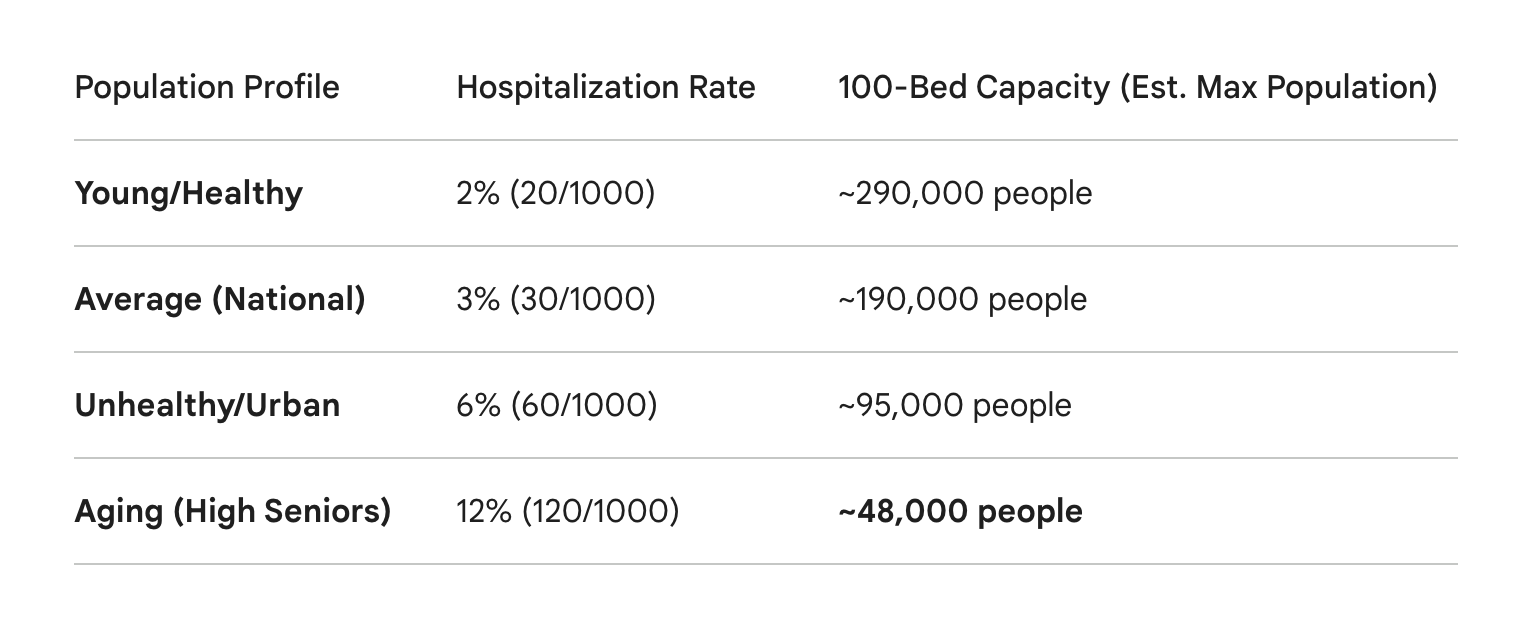
In India, the national average hospitalization rate is typically estimated at 29 to 33 per 1,000 population per year. This translates to roughly 3% of the population requiring inpatient care annually.
When we say a 100-bed hospital can serve 50,000 people, we are using the following mathematical logic:
Total Annual Bed Days: 100 beds X 365 days = 36,500 bed days.
Target Occupancy (80%): You never want a hospital 100% full (for emergencies), so you aim for 29,200 available bed days.
Average Length of Stay (ALOS): If the average patient stays 5 days, the hospital can handle about 5,840 admissions per year.
Catchment Population: If 3% of your population (1,500 people out of 50,000) needs a hospital stay each year, a 100-bed hospital easily covers them. In fact, at a 3% rate, it could theoretically cover up to 190,000 people.
Note: The "50,000" figure is often used as a conservative planning baseline to account for "surge capacity" (like flu seasons or outbreaks) and the fact that specialized private hospitals often have higher admission rates than the national average.
The hospitalization rate is somewhat higher in the aging and sick population but our 100 bed hospital for 50000 people can easily handle up to 10 % hospitalization rate. Considering our community population will have a mix of all different kinds of people. Our average will easily be below the 10 % hospitalization rate that our hospitals can handle.
Most municipal planners in India aim for 2 beds per 1,000 people (which would be 100 beds for 50,000). By hitting that gold standard, we are already providing a much higher level of service than the national average (which is closer to 0.5 to 1 bed per 1,000 in many areas).
The Fact: Private hospitals in India actually handle 60% of all hospitalizations and nearly 78% of all OPD visits, despite having only about 62% of the beds. So the crowd distribution in private and government hospitals are nearly identical.
The national average is 1.3 beds per 1000 people. This includes the private hospitals. So with the ratio of 2 beds per 1000 people. The crowd at our hospitals will be less than the average crowd at normal private hospitals. This will be more of a premium and luxury experience. Better than even private hospitals.
It is likely that at 50000 people we may feel that hospital capacity is underutilized. In that case we can open 20000 more memberships. But it's better to prepare for higher capacity at the beginning. We may scale but not downgrade capacity later.
It is estimated that the cost of construction of a 100 bed NABH hospital in the city of Pune for 2026 would go around 100 Crores which is about 1 crore per bed.
This includes the land cost of 20-25 crores. In Pune land is expensive so we have to account for the budget for land also.
This is a budget for a standard hospital with all essential healthcare facilities. Not too low and not too high.
If a 100 bed hospital can serve 50000 people. We need an investment (CAPEX) of 100 crores per 50000 people.
So this comes down to Rs. 20000 per person. We recover this from the one time Joining fee for one person.
In the previous topic we studied the total funding required for the hospital construction. In this article we will study how much each member will have to contribute and how the membership will be handled.
If a 100 bed hospital can serve 50000 people. We need an investment (CAPEX) of 100 crores per 50000 people.
So this comes down to Rs. 20000 per person. We recover this from the one time Joining fee for one person.
After 50 years the hospital would go under redevelopment. So we will need to raise fresh investment at that time. Therefore the membership validity should be limited to 50 years. After 50 years the membership will have to be renewed at the new cost. The cost will be equal to the new membership cost at that time. Calculated based on the cost of hospital construction at that time.
Sometimes people might be required to leave the city or they may want to leave the community for any reason. Therefore we must allow the members the option to transfer the membership.
A member can transfer its membership to another member. So when the transfer takes place, how do we calculate the transfer cost? Let us see.
If today a membership cost is Rs. 20000 after 5 years the new membership cost may jump to 25000 considering inflation and the fact that cost to build hospitals is going up every year due to inflation. This is just a hypothetical scenario to keep the calculations simple. This is not a real world example. In the real world the price increases may not be so high. The increase can even be zero if inflation remains zero.
So after 5 years the 90 % (45 years) of the membership validity would be remaining. Assuming full membership validity of 50 years.
The cost of membership for remaining 45 years will be
0.90 x 25000 (New membership cost) = 22500
So the old member will transfer the membership to the new member at the cost of 22500. Which is actually higher than the cost of original membership. So the old member actually ended up earning Rs. 2500 on his membership. This 2500 is due to devaluation of currency due to inflation. And it's legitimate.
Currency loses its value when we account for inflation. So it's normal and natural. And this is not an earning, this is compensation for the loss of value of currency.
It should be noted that this extra 2500 earned belongs to the old member and not the hospital. It should also be noted that this 2500 increase is caused by inflation and rising cost of hospital construction. Not the land value appreciation.
We don't compensate members for increases in land value beyond normal inflation. Because land prices can rise unexpectedly due to development in the city which can go beyond inflation. We don't compensate for that. Because we are a nonprofit entity. And generating speculative earnings does not align with the values of our organization.
It should be noted that the cost of increase in membership should only be due to inflation. If the rate of inflation is zero for a few years and the cost of building new hospitals remains the same. Then membership costs will not increase.
An increase in the membership cost is allowed only to compensate for inflation to compensate for the rising cost of hospital construction. The increase in membership cost for other reasons should not be allowed.
The membership cannot be traded in the open market the way company shares are traded. Therefore we will have an app based transfer where membership will be transferred only by the computerized system. Where the identity of the old member (Wanting to transfer) and identity of the new member (asking for membership) will remain anonymous.
People should not be allowed to transfer the membership to each other openly. This will create a black market where people will start trading memberships like company shares. Which is something we don't want. Because it does not align with our Nonprofit Cooperative values.
Note : This article is incomplete and yet to be added. In this article we will study healthcare models across the world and their pros and cons. So that we can pick the best features from these systems and adopt them into our system.
Kaiser Permanente - United States
Health Partners - United States
Unimed Brazil
Sakhi, India
HeW CO-OP (Japan)
Scias (Spain)
Shrusha Mumbai, India
Note : This article is incomplete. In this article we will study the various designs of the healthcare design for the city. We will take a deeper look at hub and spoke model. And why we choose this model for our city.
Hub and Spoke Model
In this article we discuss the approximate timeline for project funding and construction of the hospital. Please note that this is an approximate estimate. The actual time may differ but all updates will be shared transparently with members.
In this phase we will be spreading awareness and raising funds.
We will be having regular weekly offline meetups where members will discuss their concerns and their expectations. And learn about the system.
Members can give suggestions to further improve the system & our plan. Members don’t have to make any financial commitment until they are ready. We do have professionals who will be helping us in the planning, construction and design. But members are welcome to give their suggestions.
Because we are a community all decisions will be taken democratically.
The community stays in touch on our mobile app. Where members can have online discussions, vote for decisions, schedule offline meetups, track finances and more on our mobile app.
We will be raising rupees 50 crores minimum. Each member contributes minimum of 20000 so we will need about 25000 members.
We need a minimum of 50 crores investment because below 50 crores the funds will not be enough to cover the entire city. To build a decent small scale healthcare system for the city we need a minimum budget of rupees 50 crores.
In this phase members can pay one time contribution which is the member share capital. But their money is not yet locked which means that they can take their money back & leave the community anytime they want.
Payments, Refunds & membership will be managed on our mobile app. So there is no paperwork and everything is hassle free. Members will also receive financial updates on our mobile app. Where all the financial stats will be shared with the members transparently.
After raising 50 crores from 25000 members. We will enter a funds lock-in stage.
After we reach the funds lock-in phase the hospital construction begins. Therefore after funds lock-in if someone wants to leave the community and get their refund of their share capital. They will have to wait until a new member joins. Their membership will be transferred to the new member and they will get a refund.
We will also apply for NCDC (National Cooperative Development Corporation) Loan for 50-100 crores. This will give us a total of 100-150 crores in funds. And with 100 crores in hand we will acquire the land & begin the construction of the Hospital.
In this phase new members can continue to join and we can use that funds to return the loan earlier than its due date. Or if there is no loan then we can use that funds to further expand the capacity of the system.
“Sarovah Healthcare” mobile app has a finance tracking feature where members will be able to see how their funds are spent with proper Photo and Video Evidence.
The members will receive regular updates about hospital construction. On our “Sarovah Healthcare” Mobile app.
The weekly offline meetups and discussions will continue. Members are encouraged to actively participate in the process.
Timeline for phase II - After funds lock-in it will take approximately 6 months to 1 year for the hospital to open for the first patient.
We are expecting that the construction of the hospital will take 6 months to 1 year. So after 1 year the hospital is likely to open for the first patient.
Meanwhile new members can continue to join and the healthcare infrastructure will continue to expand organically to accommodate new members.
Members can continue to vote for decisions, and track hospital finances with photo and video evidence on “Sarovah Healthcare” mobile app.
In this article we will discuss various option for raising funds.
Each member makes a one time contribution. In legal terminology we call it share capital contribution. We already discussed how a member can make one time contribution of Rs. 20000 which will give us good enough CAPEX funds enough for the construction of hospitals.
One time Contribution - Share capital contribution remains the primary method for raising funds but there are few other ways also we can raise funds for our initiative. Which might be needed in different scenarios.
Besides making a share capital contribution members can also give loan to the cooperative at low interest rates. If a cooperative takes a loan from outside they will get a loan at 11 % interest rate. But members can give a loan on 7 % interest. This is a win-win for both. Members who give loans will get good return on their investment and cooperative also gets loans on cheap and low interest rates.
Well someone might ask if the one time share capital contribution from the members gives us enough money for the construction of hospitals why should we need a loan ?
We will see that in real world situations we can have various scenarios where loans might be required.
We can have a scenario where we might have planned a hospital construction budget of Rs. 100 crores from 50000 members. But it is possible that right now we have only 30000 members who contributed Rs. 60 crores. In this scenario we will have to wait for more time to raise remaining Rs. 40 crores. In such a situation it would be better to raise that 40 crores from a loan and return that loan when we get remaining 40 crores from remaining 20000 members.
Time is a valuable asset. If the construction of the hospital gets delayed too much then people may lose interest. So starting the construction ASAP even with a loan is better than delaying too much. When the construction of the hospital begins it will become easier to attract new members because when people see the progress on the ground they are more interested.
Employers provide health cover to their employees. Right now they have tie ups with various hospitals and even have group health insurance. They can make a share capital contribution on behalf of their employees.
If an employer has 100 employees that employer will make a share capital contribution of Rs. 20 lakh assuming per member share capital contribution is Rs. 20000.
This gives an employer the benefit of 50-70 % savings in their hospital costs. They can recover their investment in just few years due to savings in hospital bills. So this makes it a very attractive option for employers. They can also opt for annual subscription for their employees where they can get annual health cover for Rs. 10000 per annum per employee.
NCDC (National Cooperative Development Council) setup by government of India is highly supportive of cooperative initiatives. If we are able to raise 50 crores from members they can easily fund remaining 50 crores from loan from NCDC.
A lot of companies and corporations have a dedicated funds allocated for CSR activities. It is possible that they might consider this initiative for their CSR funds.
Government has lot of interest in providing better healthcare for citizens. They might help this initiative with grants, loans or any other ways.
If this initiative proves to be very effective we can receive supports and grant from various other sources.
It is easy to trust a healthcare initiative when you see a fully functional working hospital giving quality ethical and affordable healthcare. But trusting the initiative when we are in our infancy and yet to begin the construction of the hospitals is not easy.
So members who made their contribution when we are still in our baby phase when we are yet to start the construction of the hospital deserves special appreciation.
First 50000 members who join this initiative will be termed as founding members. And they will receive special appreciation from the community.
Listing here the suggestions of various ways we can appreciate their contribution.
Lifetime Recognization and Certification of Appreciation
Founding members will be given a Certificate of Appreciation which provides them a lifetime recognization as the founding member of the community.
5 % extra discount in their hospital Bills
We can give 5 % extra discount in the hospital bills to the founding members capped at the total lifetime benefit value of 30000 rupees. This means they save Rs. 30000 extra in their hospital bills which are already 50 - 70 % lower than private hospital bills.
Other Ways to Appreciate
Members are welcome to give their own suggestions. You’re free to suggest any other ways to appreciate their contribution.
You may have various questions about the system let us discuss them here. If we fail to address your question here feel free to reach out to us. Look in the social media and outreach to get in touch.
Question : When I join this system will I get access to just one hospital or multiple hospitals
Answer : Sarovah Healthcare is a decentralized ecosystem of multiple independent communities. One community for every village / town / city. Each community can have multiple hospitals.
When you become a member of one community you get access to all the hospitals in the ecosystem. It is because the communities have collaboration agreement with each other.
Question : How can an average person be the owner of hospitals when he has no knowledge of how healthcare works ?
Answer : An average person can own a car when he has no knowledge of how the car works. It is because when he goes to the service center to repair the car he is guided about various aspects. Yes cheating can happen in the service center but if you have a friend who is a car mechanic he can protect you from cheating and guide you in the right direction.
The average person does not need to know how to repair his car. He only needs to know who to trust and how to approve the funds. In a very similar way the average person does not need to have any technical knowledge of how hospitals work. He only needs to know who to trust and vote for policy decisions.
In our system an average person owns the healthcare system. But that person is guided by the healthcare professionals, doctors and industry veterans. An average person does not need a working knowledge of the healthcare industry. He can vote for policy decisions even without this knowledge. Because he is guided properly by the people who have this knowledge.
The community will have doctors, and healthcare workers also as members of the community. Like other members they are also concerned about their own health and the health of their own family members.
Even if an average person fails to find any problem when things are going wrong. These people can detect problems and notify and educate others about those problems.
Question : The system works very similar to how a democratic government works. There is a huge corruption in government and people’s demands are often ignored. How can we ensure that we don’t end up becoming like that ?
Answer : Problems in one democratic government do not imply the entire system of democracy is problematic. Many countries in Europe are democratic but they have negligible corruption and high accountability.
A lot depends on how the democracy is implemented.
We embrace technology to manage our community. The members can vote for decisions on their mobile app. They can organize offline meetups. Discussions within the community happen on our mobile app also.
We have a policy that each and every financial transaction is supported by a proper photo and video evidence accessible to members through the mobile app.
Because the members can vote from the comfort of their mobile phones. They can easily participate in the voting process. The management cannot force non-democratic decisions on the members. The management is only there to guide you and implement the decisions made by the community. The management has no legal authority to force its decision on the community because they don’t own the system. They are just the employees not the owners.
Because all the financial transactions are supported by a proper photo and video evidence which will be available on the mobile app for the members. The members can investigate for the possibility of corruption. And this makes the corruption very difficult or negligible.
Corruption thrives in the Government because citizens are kept in the dark and citizens have no idea how their tax money is being spent.
We are also working with the legal system to bring the ability to elect the community management through the mobile app. If the community feels a person in the management is corrupt they can remove the person by voting on the mobile app.
The corruption thrives in the government because they don’t have a policy to remove the corrupt employees. Corrupt employees mostly get transferred or suspended. But they are rarely removed from the job. So there is no fear of corruption.
This is not a problem with cooperative because cooperative laws allow the cooperative to remove the employees similar to how they can be removed from any private company. If the community finds that a certain employee or a person in management is corrupt they can remove them easily with a notice period.
Question : Can I learn, explore and experience the system before I make any payment ?
Answer : Yes you can join our community and participate in our weekly offline meetups free of cost. We organize weekly meetups in the city so that new members can learn about the system.
New members are also allowed free visits to our hospitals and healthcare facilities.
Once you are satisfied with system and want to join you can make a payment to become a member.
Sarovah Healthcare works on a decentralized healthcare model. Anyone can create a community for their village / town / city. And be the part of our ecosystem.
Each community is an independent legal cooperative with its own management, elections and finances. But they will be assisted by the ecosystem in each and every stage.
If you want to create a community in your city / town / village we are happy to provide all the help and guidance required to get started.
You can get in touch with us. See the social media and outreach section.
Sumeet graduated in computer science from university of pune in 2010. He has more than 10 years of experience working as an small business entrepreneur in the software industry.
Sumeet has deep interest in sustainable economics, cooperatives, nonprofits and how to build ethical ecosystems for the people. In 2011, Sumeet authored “Social Life and Economics” : a book on sustainable economics where he explores nonprofits, and ethical economic systems.
He also has deep interest in finding how to make healthcare ethical and affordable for people. The concept of nonprofit healthcare cooperative is a part of his broader vision for the economy where he sees nonprofits and cooperatives playing a greater role in the economy.
Sumeet loves to work with communities. In 2016 Sumeet founded an open source software project where he led and worked with an International community of open source contributors.
In 2019 his open source project gained international recognition and was featured by Y-Combinator — a premier startup incubator responsible for launching global startups like Airbnb, Stripe and Dropbox.
Despite having deep interest in technology he feels huge misalignment with the startup world where profits of the corporations become primary and concern of the people and the community take a backseat.
Working with nonprofits and cooperatives may look like a decision based in altruism but he says it’s not altruistic because he is doing it for his own selfish reasons as he enjoys working with the community and he loves his peace of mind which cannot be guaranteed in the world of startups.
Social Media
Instagram : @sarovah.health
Twitter (X) : @sarovahhealth
Email and Website
Email : reach@sarovah.health
Website : https://sarovah.health
Head Office
Pune, India